While I'm very happy to get to the first dorsal forearm post, let me first apologize for the long hiatus I've inadvertently taken. In addition to teaching at the American Academy of Art, I am also on the part time faculty at the Biomedical Visualization program at the University of Illinois at Chicago, a fabulous graduate program for future medical illustrators, animators, and anaplastologists. Although it's kept me from my blog for the past few weeks, I've very much enjoyed reading and editing many compelling research papers that this year's graduating BVIS students are finishing up. I can't give away their content, but let's just say it's amazing to see what can be done with MRI data and 3D modeling and animation applications!
The dorsal forearm is one of my favorite lectures, as its intricate and complex musculature is unmatched anywhere else in the body. At the Academy, we devote three entire classes to just the forearm; it deserves a slow and thorough explanation. I can't fit even the dorsal side into one post here, so I'll be dividing it up into a few.
Muscles in the limbs are categorized into groups (which are defined by function) that reside in muscle compartments (which are defined by location.) The forearm has two muscle compartments, the dorsal compartment (in which the extensor/supinator muscle group resides) and the ventral compartment (in which the flexor/pronator muscle group resides.) I wish I could say the dorsal and ventral compartments were placed perfectly dorsally and ventrally on the arm, but alas, they are not. Each spills over onto the other side a bit. This means while most extensor/supinators are seen on the dorsal side of the arm, a few can be seen peeking over onto the ventral side, and while most flexor/pronators are seen on the vental side of the arm, a few can be seen peeking over onto the dorsal side.
Have I lost you yet? Agh, I know this verbal explanation is really dry, so lets try a diagram. Click for an enlarged view if necessary!

Above we see dorsal (top side) and ventral (underside) views of the right forearm. We also see the location of the extensor/supinator muscle group (shown in blue) and the flexor/pronator muscle group (shown in green.) Notice how we see mostly extensor/supinators on the dorsal side, but a few flexor/pronators creep over there. Similarly, we see mostly flexor/pronators on the ventral side, but a few extensor/supinators creep over there. It's like they each know where their home is, but they can't resist peeking around to the other side.
Since the two forearm muscle groups are not clearly divided between the ventral and dorsal sides, we use other landmarks to find their borders. On the dorsal side of the arm, the crest of the ulna (the distal end of the bone that can be seen and felt on the surface of the arm) is the border between the two muscle groups. On the ventral side, the biceps brachii tendon (coming from the biceps brachii muscle on the anterior upper arm) is the border between the two muscle groups.
When observing the muscles of the forearm, the best way to become oriented is to first figure out where the two muscle groups (and the borders between them) are. As such, when observing the dorsal forearm, the first structure we want to identify is the ulnar crest. This actually doesn't look like much on the surface, but it's easy to find A) because we can usually feel it, and B) because it merges with a nice little furrow at its proximal end.

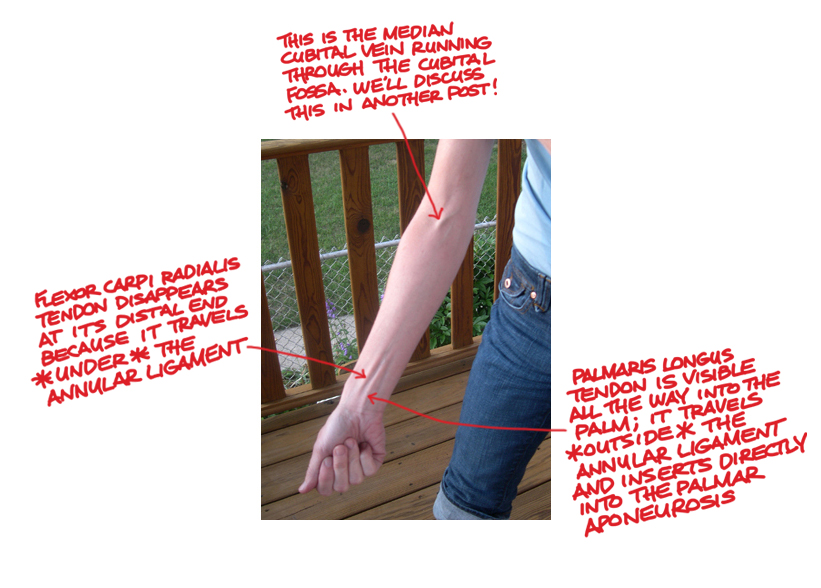
In the above photograph, the arrow is pointing to the crease along the ulnar crest. Everything above this in the photograph is the extensor/supinator group, and everything below this is the flexor/pronator group.

In this photo, the dashed line follows most of the furrow along the ulna distally until we reach the head of the ulna (the little bump on the pinky side of the wrist. The furrow stops suddenly at its proximal end because at that point we run into the anconeus muscle, a small triangular muscle between the lateral epicondyle of the humerus and the olecranon process of the ulna (what we normally think of as the elbow.)
 |
| The area in blue (above the red dashed line) is the extensor/supinator group. The area in green (below the red dashed line) is the flexor/pronator group. Muscles are outlined and labeled: BRR (brachioradialis); ECRL (extensor carpi radialis longus); ED (extensor digitorum); EDM (extensor digiti minimi); ECU (extensor carpi ulnaris); Anc (anconeus); and FCU (flexor carpi ulnaris) which is the only muscle from the flexor pronator group that can be seen from this view. |
In the above image, we can still see the division between the two muscle groups (shown with a red dashed line) but we can also see outlines of muscles within each compartment. Notice how the division line runs right along the ulnar crest and ends distally at the head of the ulna. Notice also how the proximal end of the division line ends at the triangular anconeus muscle.
Now that things are a little more clarified, lets revisit the unembellished arm photo and take another look at the muscles shapes.

So I think that's all we'll cover for today. Keep in mind that these early posts tend to show the body in odd positions because we are still covering straightforward anatomy, and these positions are meant to help pronounce all structures in a given area. Later on we'll observe the arm (and the rest of the body) in more natural poses and note what structures are seen then.
Dorsal forearm part 2 to come soon! At that point we'll look more closely at the individual muscles and learn to tell them apart. Thanks to my forearm model, Shannen!